
2022年第三期

经颅直流电刺激治疗轻度认知障碍与轻中度阿尔茨海默病疗效的系统评价分析
日期:2023-11-22
目的: 评估经颅直流电刺激用于治疗轻度认知障碍及轻中度阿尔茨海默病的疗效及安全性。方法: 检索建库至2022年3月发表在Pubmed、Embase、Cochrane Central Register of controlled Trials、ClinicalTrails.gov、中国生物医学数据库、知网、万方、维普等数据库的文章。主要结局指标为干预前后的主要认知功能变化,次要结局指标为出现的不良事件情况。采用Review Manager 5.2软件对提取数据进行分析,并使用Cochrane偏倚风险评价工具对纳入文献进行质量评价。结果: 最终纳入23项研究,其中18项研究(20个数据组)纳入定量分析,共计953人。发现经颅直流电刺激对认知功能存在改善作用(SMD=0.75, 95%CI=[0.42,1.08],P<0.00001);亚组分析提示其在轻度认知障碍(SMD=0.20,95%CI= [0.02,0.37],P=0.03)和轻中度阿尔茨海默病(SMD=0.79,95%CI=[0.53,1.04],P<0.00001)人群中均有效,优化的参数选择为单侧/双侧额颞顶叶、0.06mA/cm2的电流密度,进行≤20次刺激存在认知获益的。结论: 经颅直流电刺激有利于轻度认知障碍和轻中度阿尔茨海默病的认知改善,推荐刺激部位在单侧/双侧额颞顶叶附近,采用0.06mA/cm2的电流密度,进行较短期的治疗,有待更多的高质量研究对更高的电流密度以及延长治疗周期的疗效进行探索。
Abstract
Objective: To evaluate the efficacy and safety of transcranial direct current stimulation in the treatment of mild cognitive impairment and mild to moderate Alzheimer's disease. Methods: These articles published in Pubmed, Embase, Cochrane Central Register of Controlled Trials, Chinese Biomedical Database, CNKI, Wanfang, VIP and other Chinese and English databases before March 8, 2022 were searched, with a supplementary search of unpublished clinical trials on Clinicaltrails.gov. The primary outcome is the change of score in the main cognitive function scale before and after the intervention, and the secondary outcome was the occurrence of adverse reactions. Review Manager 5.2 software was used to summarize and analyze the extracted data, and Cochrane bias risk assessment tool was used to evaluate the quality of the included literature. Results: Twenty-three studies were included, of which 18 studies (20 data groups) were included in quantitative analysis, with a total of 953 people. Comprehensive all included study indicates the anode transcranial direct current stimulation to improve cognitive function (SMD = 0.75, 95% CI = [0.42, 1.08], P < 0.00001); Subgroup analysis suggested that was effective in both mild cognitive impairment(SMD=0.20, 95%CI= [0.02, 0.37], P=0.03) and mild to moderate Alzheimer's disease (SMD=0.79, 95%CI=[0.53, 1.04], P < 0.00001). The optimized parameters of transcranial direct current stimulation were unilateral/bilateral frontotemporal parietal lobe, 0.06mA/cm2 current density, and ≤20 times of stimulation has been proved to have cognitive benefits. Conclusion: Transcranial direct current stimulation is safe and effective for the treatment of cognitive impairment in mild cognitive impairment and mild to moderate Alzheimer's disease. According to current research data, the recommended stimulation site is unilateral/bilateral frontotemporal parietal lobe, and 0.06mA/cm2 current density is used in a short-term treatment. More high-quality studies are needed to explore the benefits of higher current densities and prolonged treatment cycles.
关键词
经颅直流电刺激 / 轻度认知障碍 / 阿尔茨海默病 / 系统评价
Key words
Transcranial direct current stimulation / Mild cognitive impairment / Alzheimer's disease / Systematic review
引用本文
肖淑方 , 李佳敏 , 刘一丹 , 李小凤. 经颅直流电刺激治疗轻度认知障碍与轻中度阿尔茨海默病疗效的系统评价分析. 阿尔茨海默病及相关病杂志. 2022, 5(3): 224-232 https://doi.org/10.3969/j.issn.2096-5516.2022.03.012
XIAO Shufang , LI Jiamin , LIU Yidan , LI Xiaofeng. Effects of transcranial direct current stimul ation on mild cognitive impairment and mild to moderate alzheimer’s diseade : a systematic review and meta-analysis. Chinese Journal of Alzheimer's Disease and Related Disorders. 2022, 5(3): 224-232 https://doi.org/10.3969/j.issn.2096-5516.2022.03.012
前言:
阿尔茨海默病(Alzheimer’s Disease, AD)是一种神经变性疾病,早期典型临床表现为情景记忆损害为主的记忆力障碍,缓慢进行性加重,或可伴精神行为异常等表现,目前尚无明确的可改变疾病进程的治疗方法[1]。随着人口老龄化进程加快,AD越发受到关注,而轻度认知障碍(Mild Cognitive Impairment, MCI)介于认知功能轻度受损和痴呆之间,受累及的认知领域较单一,日常生活能力无明显受损,故可把MCI作为预防痴呆的重点[2]。
经颅直流电刺激(Transcranial Direct Current Stimulation, tDCS)通过局部微电流无创刺激大脑皮层,其阳极刺激增加皮层兴奋性[3],并引起钙依赖性的谷氨酸神经元突触可塑性改变及 γ-氨基丁酸相关的谷氨酸能神经元活动增加[4] ,产生相关的脑区功能改变。tDCS被广泛研究应用于神经系统领域,涉及疼痛、帕金森病、脑卒中、AD、抑郁症、药物成瘾等的治疗[5],具有便捷、安全等优点。
研究表明tDCS可对认知各个领域起改善作用[6⇓⇓⇓-10],同时也有研究表明未见tDCS治疗对认知障碍患者产生积极影响[11⇓⇓⇓-15],相关Meta分析[16-17]提示阳极tDCS对于认知改善均存在积极作用;另有荟萃分析[18]认为对整体认知功能有改善作用的是重复经颅磁刺激而非tDCS。此次纳入新近的临床研究进行分析,以进一步探索tDCS对MCI及轻中度AD患者的疗效。
1 方法
本文遵循《系统综述和荟萃分析优先报告的条目: PRISMA声明》进行阐述[19]。
1.1 检索策略
计算机检索PubMed、Cochrane Central Register of controlled Trials、Embase、中国知网、万方医学、维普、中国生物医学文献数据库等中英文数据库2022年3月8日前发表的随机对照试验,并对ClinicalTrial.gov进行补充检索未发表的随机临床试验及人工检索相关文章参考文献。英文数据库进行主题词+相应自由词检索,主题词均为“Transcranial Direct Current Stimulation、Alzheimer disease、Cognitive Dysfunction”,中文数据库进行“经颅直流电刺激、阿尔茨海默病、轻度认知障碍”等关键字进行中英文及同义词扩展检索,并由两位作者遵循以下的纳入排除标准分别筛选,如遇见意见不一致,则进行讨论,仍有争议则由第三人进行评定。
1.2 纳入标准
1.2.1 研究对象
依据国内外痴呆与认知障碍诊断指南[20-21]或其他普遍认可的专家共识进行诊断的MCI和(或)AD患者为研究对象,其中MCI患者为有记忆力减退主诉,客观量表检查等存在认知域受损,但未达到痴呆诊断标准,日常生活能力未受损;纳入的轻中度AD患者为达到痴呆诊断,依据简易智力状态检查量表(MMSE)、临床痴呆量表(CDR)等评估达轻中度痴呆的患者(文盲MMSE≥9分,非文盲MMSE≥10分,或CDR为1~2分)。
1.2.2 干预措施
试验组采用阳极tDCS、对照组采用假tDCS对特定脑区进行单次或重复多次刺激,且允许同时合并其他干预措施。
1.2.3 结局指标
研究至少包含基线及治疗终点时的认知相关神经心理学测试或其他评估任务结果,不对采用的测试种类、涉及认知领域等进行限制。结局指标采用的表达方式为平均值±标准差,或者其他可以转化为平均值±标准差的表述形式也被接受。
1.2.4 研究设计
纳入研究均为随机对照试验,包括平行对照试验、随机交叉试验等。
1.3 排除标准
排除其他类型痴呆、其他神经精神类疾病以及特殊感染、全身系统性疾病等所致的认知障碍。同时排除纳入重度AD患者以及仅纳入健康志愿者的研究。排除不可获取全文的研究。
1.4 数据提取
两位作者各自进行数据提取,结局指标选取研究的主要结局指标或根据文章分析更能提示全面认知领域情况的量表指标作为主要结局指标。次要结局指标为不良事件发生情况。对于图表型数据采用GetData Graph Digitizer 2.26进行数据提取,对文章未提供数据向原作者请求获取,以上方法均不能获取所需数据时,则相应研究从定量分析中排除。
1.5 文章质量评价
两位作者依据Cochrane偏倚风险评价工具的标准对所纳入文章独立进行质量评价,当出现异议时由第三人进行裁决。
1.6 数据分析
研究采用Review Manager 5.2软件对提取数据进行效应量合并分析。纳入研究选取治疗终点与基线主要认知量表评估分数差值的均值±标准差进行数据分析,因评估指标均为连续型变量,且不同研究结局指标不同,故选取标准化均数差(Standardized Mean Difference, SMD)及其95%置信区间(confidence interval,CI)作为效应指标,纳入研究的样本量不足,且异质性较大,选取随机效应模型作为分析模型。采用I2作为异质性检验指标,对于I2>50%的情况进一步进行亚组分析及敏感性分析,评估异质性来源,以对结果做出解释。对纳入研究采用漏斗图进行发表偏倚评估。
2 结果
2.1 一般研究特征
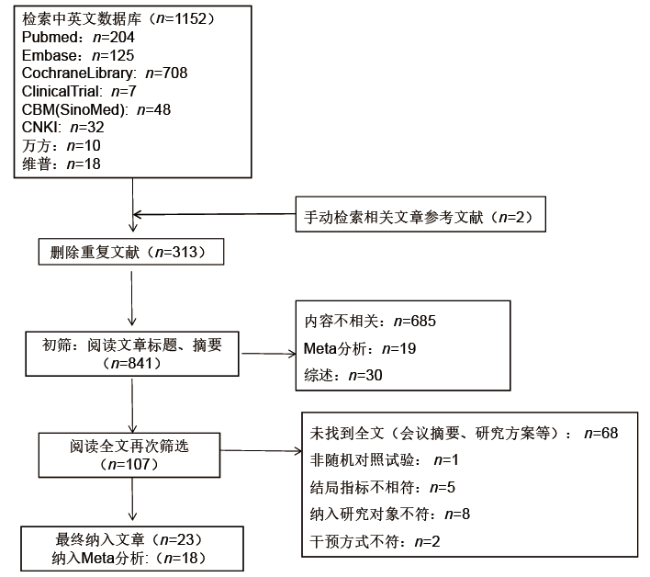
经检索共获取文献1154篇,去除重复文章313篇,通过阅读题目、摘要及查找并阅读全文后;最终本系统评价纳入23项研究,纳入定量数据分析的文章为18篇。具体纳入研究筛选流程详见图1。
纳入23项研究,共计1062人;纳入定量分析18项,其中有2项研究数据提取2次,共计20个数据组,总人数为953人。具体特征及tDCS刺激参数情况详见表1。10/18的研究纳入的主要结局指标均是对整体认知功能(MMSE[11,22⇓⇓⇓ -26]、MoCA[7,27]、CAMCOG[8]、BMDB[28])评价,4/18为记忆力(WRT[10]、VRT[9]、FNAT[15]、CVLT-II[12])评估,4/18为工作记忆(DST-f[29- 30]、N-back[31]、VSA-RVP[32])评估。
表1 纳入研究一般特征Tab.1 General characteristics of included studies |
| 纳入研究 | 地区 | 纳入人群 | 教育程度(年) | 年龄 (岁) | 性别 (男/女) | 研究设计 | 干预措施 | 刺激部位 | 电流(mA) | 电流密度(mA/cm2) | 刺激持续时间 | 刺激次数 | 结果 | 失访人数 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ferrucci 2008 | 意大利 | 可能的AD | 10.9±4.8 10.9±4.8 | 75.2±7.3 75.2±7.3 | 3/7 3/7 | RCT | 阳极tDCS 假tDCS | 双侧颞顶区各15min | 1.5 | 0.06 | 30min | 单次 | 可改善AD单词再认记忆 | 4 |
| Boggio 2012 | 意大利 | AD | 14.4±3.7 14.4±3.7 | 78.9±8.1 78.9±8.1 | 8/7 8/7 | RCT | 阳极tDCS 假tDCS | 双侧颞叶 | 2 | 0.06 | 30min 连续5天 | 5次 | 能改善AD视觉识别记忆 | 0 |
| Cotelli 2014 | 意大利 | 可能的轻中度AD | 5.5±2.4 8.9±5.1 | 76.6±4.6 74.7±6.1 | 2/10 3/9 | RCT | 认知训练+阳极tDCS 认知训练+安慰剂tDCS | 左侧DLPFC | 2 | 0.08 | 25min 5次/周,2周 | 10次 | 无影响 | 4 |
| Khedr 2014 | 埃及 | 可能的轻中度AD | NM | 68.5±7.2 67.3±5.9 | 6/5 5/6 | RCT | 阳极tDCS 假tDCS | 左侧DLPFC | 2 | 0.08 | 25min 连续10天 | 10次 | 可改善整体认知功能 | 0 |
| 胡荣亮 2016 | 中国 | aMCI | 8.7±3.7 8.4±4.3 | 67.9±5.3 68.3±3.7 | 12/6 13/8 | RCT | 阳极tDCS 假tDCS | 右侧小脑 | 1.2 | 0.03 | 20min 连续5天 | 5次 | 可改善言语工作记忆能力 | 0 |
| 王东 2016 | 中国 | AD | NM | 67.3±5.9 68.5±7.2 | 36/24 34/26 | RCT | 阳极tDCS 假tDCS | 左侧DLPFC | 2.5-5 | NM | 25min 连续10天 | 10次 | 可改善认知功能 | 0 |
| Gomes 2019 | 巴西 | MCI | NM | 73.0±9.2 71.6±7.9 | 9/20 7/22 | RCT | 阳极tDCS 假tDCS | 左侧DLPFC | 2 | 0.08 | 30min 2次/周,5周 | 10次 | 可提高记忆力、语言流畅性和执行功能 | 0 |
| Im 2019 | 韩国 | 早期可能的AD | 6.3±3.8 5.4±5.9 | 71.9±9.2 74.9±5.0 | 1/10 2/5 | RCT | 阳极tDCS 假tDCS | 左侧DLPFC | 2 | 0.07 | 30min 6个月 | 180次 | 可改善整体认知功能和命名 | 2 |
| Khedr 2019 | 埃及 | 可能的轻中度AD | 4.0±2.8 3.5±2.0 | 64.2±3.6 65.2±4.5 | 13/10 13/8 | RCT | 阳极tDCS 假tDCS | 双侧颞顶叶各20min | 2 | 0.06 | 40min 5次/周,2周 | 10次 | 整体认知功能改善 | 2 |
| lu 2019 | 中国 香港 | 轻度认知障碍(AD) | 7.3±4.8 6.5±4.3 | 74.2±6.7 74.5±6.6 | 21/42 17/36 | RCT | WMT+阳极tDCS WMT+假tDCS | 左侧外侧颞叶皮质 | 2 | 0.06 | 20min 3次/周,4周 | 12次 | tDCS联合工作记忆训练可改善认知功能 | 28 |
| Martin 2019 | 澳大利亚 | aMCI | 14.5±3.5 14.9±3.2 | 71.8±6.4 71.6±6.4 | 13/20 10/25 | RCT | 认知训练+阳极tDCS 认知训练+假tDCS | 左侧DLPFC | 2 | 0.06 | 30min 3次/周,5周 | 15次 | 未产生更显著的记忆改善 | 13 |
| 徐颖2019(1) | 中国 | MCI | 10.4±2.8 10.0±2.9 | 59.5±5.4 61.8±6.5 | 7/32 13/26 | RCT | 太极拳+阳极tDCS 太极拳+假tDCS | 右侧DLPFC | 2 | NM | 20min 3次/周,12周 | 36次 | 太极拳联合tDCS改善MCI患者整体认知功能和注意力 | 13 |
| 徐颖2019(2) | 中国 | MCI | 8.7±3.0 8.7±3.0 | 60.3±7.3 58.2±5.4 | 20/19 14/25 | RCT | 健步走+阳极tDCS 健步走+假tDCS | 右侧DLPFC | 2 | NM | 20min 3次/周,12周 | 36次 | 注意力改善 | 17 |
| Fileccia 2019 | 意大利 | MCI | 10.5±4.1 11.5±3.7 | 71.6±5.8 69.7±6.6 | 13/4 11/6 | RCT | 阳极tDCS 假tDCS | 左侧DLPFC | 2 | 0.06 | 20min 5次/周,4周 | 20 | 对MCI认知改善有益 | 0 |
| Stonsaovapak2020 | 泰国 | MCI | NM | 68.4±8.4 69.7±7.6 | 2/21 2/20 | RCT | 阳极tDCS 假tDCS | 右侧DLPFC | 2 | 0.08 | 20min 3次/周,4周 | 12次 | 可改善认知功能 | 1 |
| 胡荣亮 2020 | 中国 | aMCI | NM | 64.1±3.4 65.0±3.8 | 12/8 11/9 | RCT | 阳极tDCS 假tDCS | 左侧DLPFC | 1 | 0.11 | 20min 5次/周,2周 | 10次 | 可提高言语工作记忆能力 | 0 |
| Gangemi 2021(1) | 意大利 | 轻度AD | 6.5±2.0 6.1±2.1 | 67.5±2.8 69.0±3.1 | 10/16 | RCT | 阳极tDCS 假tDCS | 左侧额颞叶 | 2 | 2.5 | 20min 10天 | 10次 | 减缓AD病程 | NM |
| Gangemi 2021(2) | 意大利 | 轻度AD | 6.7±2.0 6.2±2.7 | 68.5±2.8 68.7±3.1 | 5/13 | RCT | 阳极tDCS 假tDCS | 左侧额颞叶 | 2 | 2.5 | 20min 10天/月 8个月 | 80次 | 减缓AD病程 | NM |
| Gonzalez 2021 | 中国香港 | MCI | 9.7±3.6 9.7±3.6 | 69.8±5.3 71.0±6.2 | 6/15 8/16 | RCT | 认知训练+阳极tDCS 认知训练+假tDCS | 左侧DLPFC | 1.5 | 0.1 | 30min 3次/周,3周 | 9次 | 提高了任务特异性结局的处理速度 | 3 |
| He 2021 | 中国 | MCI | 10.4±3.1 9.0±2.5 | 63.5±4.8 65.6±3.5 | 7/17 4/15 | RCT | 阳极tDCS 假tDCS | 左侧DLPFC | 1 | NM | 20min 5次/周,2周 | 10次 | 无效 | 0 |
| Rodella 2021 | 意大利 | MCI | 11.1±5.0 9.7 ± 5.0 | 71.6±5.7 75.1±4.8 | 8/5 9/6 | RCT | CoRE+阳极tDCS CoRE+假tDCS | 左侧DLPFC | 2 | 0.125 | 30min 4次/周,3周 | 12次 | 对整体认知功能无显著影响 | 5 |
| Suemoto 2014 | 巴西 | 可能的中度AD | 5.0±4.2 4.5±3.9 | 79.4±7.1 81.6±8.0 | 5/15 7/13 | RCT | 阳极tDCS 假tDCS | 左侧DLPFC | 2 | 0.06 | 20min 3次/周,2周 | 6次 | 无明显改善作用 | 0 |
| Bystad 2016 | 挪威 | 可能的AD | NM | 70.0±8.0 75.0±8.7 | 7/5 7/6 | RCT | 阳极tDCS 假tDCS | 左侧颞叶 | 2 | 0.06 | 30min 10天 | 6次 | 无明显改善 | 1 |
| Yun 2016 | 韩国 | MCI | 8.1±4.9 5.6±2.4 | 74.8±7.5 73.1±4.3 | 3/5 2/6 | RCT | 阳极tDCS 假tDCS | 左侧DLPFC | 2 | 0.08 | 30min 3次/周,3周 | 9次 | 主观记忆满意度和记忆策略的改善 | 0 |
| Das2019 | 美国 | MCI | 17.9±3.9 16.2±1.8 | 62.6±8.4 63.3±7.4 | 4/8 2/8 | RCT | SMART+阳极tDCS SMART+假tDCS | 左侧额下回 | 2 | 0.13 | 20min 2次/周,4周 | 8次 | 抑制SMART训练对抑制、创新、情景记忆等认知领域的改善 | 6 |
| Note: RCT randomized controlled trial, DLPFC dorsolateral prefrontal cortex, WMT working memory training, NM not mentioned, core cognitive training, smart reasoning training. |
2.2 纳入研究质量评价
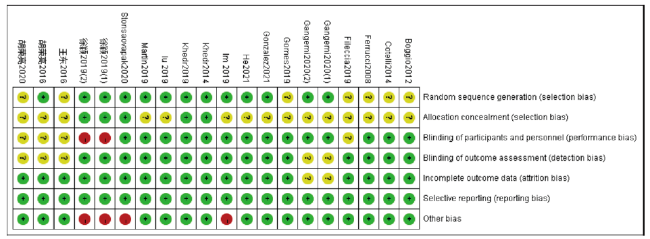
对纳入Meta分析的研究进行偏倚风险评估,结果提示7项研究对随机化方法未作明确描述[8⇓-10,15,25,28 -29];仅4项研究对随机序列的分配隐藏方法进行描述[7,23,26,32];1项研究为单盲[7], 4项研究对评估者盲法未作描述[22,25,29 -30];1项研究未报告受试者失访情况[22];其他偏倚风险中,1项研究内容与研究者存在利益关系[24],2项研究在认知基线评估中存在组间差[7,32]。详细偏倚风险评估情况见图2及图3。
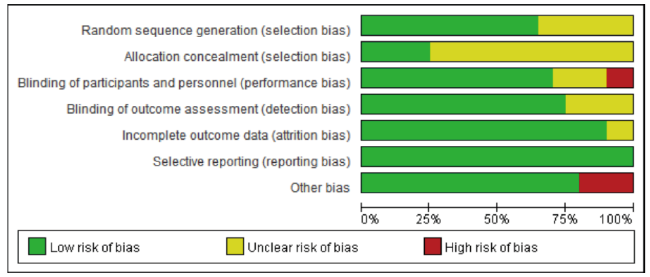
图2 偏倚风险图:对所有纳入研究产生偏倚风险项目所占百分比的判断Fig.2 Bias risk map: judgment on the percentage of all included studies with bias risk |
2.3 AtDCS VS StDCS对认知改善的作用
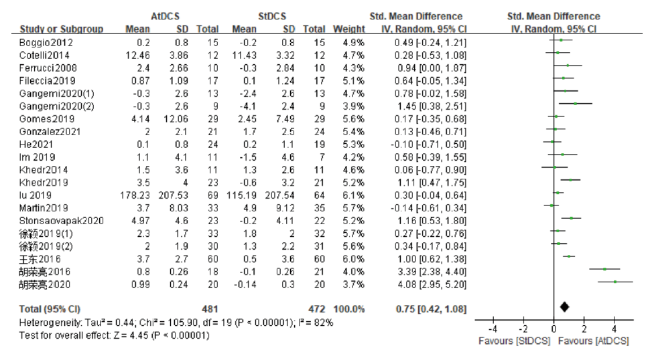
最终纳入定量分析数据组20组,共计953人,其中干预组481人,对照组471人。分析结果提示对于纳入的MCI及轻中度AD患者,阳极刺激组(Anodal Transcranial Direct Current Stimulation,AtDCS)较假刺激组(Sham Transcranial Direct Current Stimulation,StDCS)对认知功能改善存在积极作用(SMD=0.75, 95%CI=[0.42, 1.08],P<0.00001),但结果具有很大的异质性,且具有统计学意义(I2=82%,P<0.00001)。见图4。
基于刺激部位进行亚组分析,仍表明AtDCS可改善认知功能,但仅在单侧/双侧额颞顶叶亚组提示异质性下降(I2=41%, P=0.13)。对其进行敏感性分析,剔除1项研究后异质性明显下降(I2=0%,P=0.60),效应量SMD=0.91, 95%CI= [0.55, 1.26], P<0.00001[31]。
基于电流密度进行亚组分析,在电流密度为0.03、0.06、0.11、2.5 mA/cm2的亚组均可见AtDCS组治疗效果优于对照组,其中0.06 mA/cm2亚组包含6项研究,其效应量SMD=0.48,95%CI=[0.12, 0.85], P=0.01,但仍异质性较高(I2=57%,P=0.04);敏感性分析予以剔除2项研究[12,31]后异质性下降(I2=0%,P=0.60)。
基于刺激总次数进行亚组分析,≤20次与≥40次两个亚组均提示AtDCS有益于认知改善,且有统计学意义(P=0.0004,P<0.00001);≤20次亚组结果异质性高(I2=85%,P<0.00001),剔除3项研究后异质性下降(I2=33%,P=0.13)[29-30,32],且仍支持AtDCS组认知改善作用的结论。
基于纳入研究对象的认知障碍程度,分为MCI和AD两个亚组,结果均提示AtDCS具有认知改善作用(MCI亚组:SMD=0.80,95%CI= [0.28, 1.31],P=0.002;AD亚组:SMD=0.79,95%CI=[0.53, 1.04],P<0.00001),但前者异质性高(I2=89%,P<0.00001),剔除3项研究后异质性下降(I2=0%,P=0.63)[29-30,32],该结果与既往荟萃分析结果一致[16]。
以上亚组分析及敏感性分析结果汇总情况见表2。
表2 不同亚组分析及相应敏感性分析纳入研究及分析结果Tab.2 Included studies and analysis results of different subgroup analysis and corresponding sensitivity analysis |
| 亚组 | 数据组数量 | 样本量(A/S) | SMD(95%CI) | P值 | 异质性 | 敏感性分析剔除文献 | P值(敏感性分析后) | 异质性(敏感性分析后) |
|---|---|---|---|---|---|---|---|---|
| 刺激部位 | ||||||||
| 左侧DLPFC | 10 | 238/234 | 0.58(0.07,1.10) | 0.03 | 85% | 王东2016、 胡荣亮2020 | 0.26 | 0% |
| 右侧DLPFC | 3 | 86/85 | 0.55(0.04,1.07) | 0.04 | 63% | / | / | / |
| 单侧/双侧 额颞顶叶 | 6 | 139/132 | 0.73(0.36,1.09) | 0.0001 | 41% | Lu2019 | <0.00001 | 0% |
| 右侧小脑 | 1 | 18/21 | 3.39(2.38,4.40) | <0.00001 | / | / | / | / |
| 电流密度 | ||||||||
| 0.03mA/cm2 | 1 | 18/21 | 3.39(2.38,4.40) | <0.00001 | / | / | / | / |
| 0.06mA/cm2 | 6 | 167/162 | 0.48(0.12,0.85) | 0.01 | 57% | Martin2019 | 0.0003 | 30% |
| 0.07mA/cm2 | 1 | 11/7 | 0.58(-0.39,1.55) | 0.24 | / | / | / | / |
| 0.08mA/cm2 | 4 | 75/74 | 0.43(-0.09,0.96) | 0.10 | 57% | Stonsaovapak2020 | 0.39 | 0% |
| 0.1mA/cm2 | 1 | 21/24 | 0.13(-0.46,0.71) | 0.67 | / | / | / | / |
| 0.11mA/cm2 | 1 | 20/20 | 4.08(2.95,5.20) | <0.00001 | / | / | / | / |
| 2.5mA/cm2 | 2 | 22/22 | 1.02(0.38,1.66) | 0.002 | 0% | |||
| 刺激次数 | ||||||||
| ≤20次 | 15 | 338/333 | 0.80(0.36,1.23) | 0.0004 | 85% | 胡荣亮2016、 胡荣亮2020、 Stonsaovapak2020 | 0.003 | 33% |
| 20-40次 | 2 | 63/63 | 0.30(-0.05,0.65) | 0.09 | 0% | / | / | / |
| ≥40次 | 3 | 80/76 | 0.99(0.66,1.33) | <0.00001 | 0% | / | / | / |
| 认知障碍程度 | ||||||||
| AD | 9 | 164/158 | 0.79(0.53,1.04) | <0.00001 | 11% | / | / | / |
| MCI | 11 | 317/314 | 0.80(0.28,1.31) | 0.002 | 89% | 胡荣亮2016、 胡荣亮2020、Stonsaovapak2020 | 0.03 | 0% |
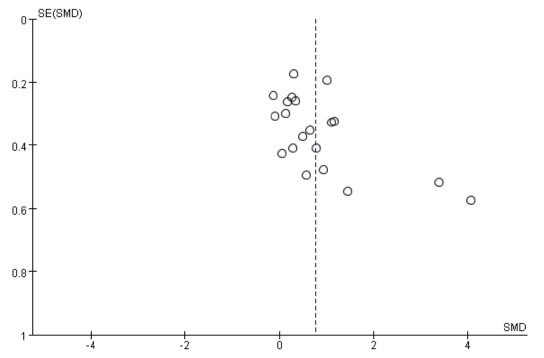
2.4 发表偏倚

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
2.5 安全性评价
3 讨论
研究表明AtDCS有改善认知的作用,其效应量SMD=0.75,但结果异质性高,亚组分析及敏感性分析发现异质性主要来源于4项研究,根据文章偏倚风险评价,其中1项研究[32]的主要认知指标存在组间基线不平衡,3项研究未报告设盲情况[25,29 -30],2项研究[25,29]未报告随机方法,上述偏倚风险可能影响结局,剔除后异质性下降(I2=29%,P=0.14),且效应量SMD=0.36, 95%CI=[0.17, 0.54],仍支持前述结论,这与此前的一项荟萃分析报告的结果一致[16]。
AtDCS可引起局部静息电位去极化,增加皮层兴奋性[3],其效应与电流密度密切相关,有研究发现AtDCS的刺激作用效果与电流强度呈非线性关系[33];又有研究表明其作用与电流密度呈正相关[34];一项荟萃分析显示增加电流密度可增加神经精神疾病患者认知任务的反应准确性[35],故而较大电流密度是否产生更强的作用效果尚不清楚,而现有数据不足以进行效应量合并分析,其效果和其中机制有待进一步探索。
一项荟萃分析提示tDCS疗效与其刺激次数呈正相关[36];而另有研究发现长期tDCS治疗可进行性地改善认知功能。此次对刺激次数进行亚组分析[37],发现在≤20次刺激的情况下AtDCS存在治疗作用(敏感性分析后SMD=0.33),而在≥40次的刺激条件下再次显现出治疗的积极作用(SMD=0.99),且效应量的值更大,有理由推测延长刺激周期、增加刺激次数可达到更佳的改善认知作用,但有待验证。
本次纳入数据组中13/20的刺激部位选择在DLPFC,尤其是左侧DLPFC(10/20),但此次发现在单侧/双侧颞叶附近存在相对可靠的疗效。早期AD的影像学研究表明,其主要的结构和功能缺陷发生在颞叶和顶叶区域[38],且颞叶前部、内侧(紧邻边缘系统)与神经功能密切相关;而DLPFC被认为参与记忆的调节,其功能与海马体-前额叶回路密切相关,但海马体到前额叶皮层存在神经纤维投射,前额叶皮层到海马之间并没有直接或间接的纤维投射[39],这一特点可能使DLPFC在认知代偿方面作用受到限制。
本研究存在一定的局限性。首先,纳入本荟萃分析的研究中多为小样本研究,部分研究存在偏倚风险。其次,纳入系统评价的研究中有5项研究[13-14,40⇓ -42]未能获取可用于荟萃分析的数据,上述数据可能对研究结局及发表偏倚等产生影响。第三,本研究数据分析大多存在很高的异质性,经亚组分析及敏感性分析后,仍无法完全明确异质性来源。最后,经漏斗图分析发现相关研究存在可能的发表偏倚,但未进一步定量评估发表偏倚情况。
4 结论
AtDCS可用于改善MCI及轻中度AD相关的认知障碍,在单侧/双侧额颞顶叶采用0.06mA/cm2的电流密度进行较短期的治疗被认为是有效的,但仍有待更多的高质量研究对更高的电流密度以及延长治疗周期的疗效进行探索。在安全性方面,AtDCS治疗未见报告严重不良事件,其不良反应均轻微、可耐受,短时间内可自行消失,故安全性尚可。
| [1] | Valencia LR, Minguez CA, Kenigsberg P, et al. Current and emerging avenues for Alzheimer's disease drug targets[J]. J Int Med, 2019, 286(4): 398-437. |
| [2] | Jia L, Du Y, Chu L, et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study[J]. The Lancet Public health, 2020, 5(12):e661-e671. |
| [3] | Nitsche M, Paulus W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation[J]. J physiol, 2000, 527(3):633-639. |
| [4] | Fregni F, Boggio P, Nitsche M, et al. Anodal transcranial direct current stimulation of prefrontal cortex enhances working memory[J]. Experiment Brain Res, 2005, 166(1):23-30. |
| [5] | Lefaucheur JP, Anta A, Ayache SS, et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS)[J]. Clin Neurophysiol, 2017, 128(1):56-92. |
| [6] | Smirni D, Oliveri M, Misuraca E, et al. Verbal Fluency in Mild Alzheimer's Disease: transcranial Direct Current Stimulation over the Dorsolateral Prefrontal Cortex[J]. J Alzheimers Dis, 2021, 81(3):1273-1283. 本文引用 [1] 摘要 |
| [7] | 徐颖. 基于多模态核磁技术探讨太极拳联合tDCS对MCI患者认知功能影响的神经机制研究[D]; 福建中医药大学, 2019. |
| [8] | Gomes MA, Akiba HT, Gomes JS, et al. Transcranial direct current stimulation (tDCS) in elderly with mild cognitive impairment: A pilot study[J]. Dement neuropsychol, 2019, 13(2):187-195. |
| [9] | Boggio PS, Ferrucci R, Mameli F, et al. Prolonged visual memory enhancement after direct current stimulation in Alzheimer's disease[J]. Brain stimulation, 2012, 5(3): 223-230. 本文引用 [3] 摘要 |
| [10] | Ferrucci R, Mameli F, Guide I, et al. Transcranial direct current stimulation improves recognition memory in Alzheimer disease[J]. Neurol, 2008, 71(7): 493-498. |
| [11] | He F, Li Y, Li C, et al. Repeated anodal high-definition transcranial direct current stimulation over the left dorsolateral prefrontal cortex in mild cognitive impairment patients increased regional homogeneity in multiple brain regions[J]. PloS One, 2021, 16(8): e0256100. |
| [12] | Martin DM, Mohan A, Alonzo A, et al. A Pilot Double-Blind Randomized Controlled Trial of Cognitive Training Combined with Transcranial Direct Current Stimulation for Amnestic Mild Cognitive Impairment[J]. J Alzheimers Dis, 2019, 71(2):503-512. 本文引用 [3] 摘要 |
| [13] | Bystad M, Gronli O, Rasmussen ID, et al. Transcranial direct current stimulation as a memory enhancer in patients with Alzheimer's disease: a randomized, placebo-controlled trial[J]. Alzheimers Res Thera, 2016, 8(1):13. |
| [14] | Suemoto CK, Apolinario D, Nakamura-Palacios EM, et al. Effects of a non-focal plasticity protocol on apathy in moderate Alzheimer's disease: a randomized, double-blind, sham-controlled trial[J]. Brain stimulation, 2014, 7(2):308-313. 本文引用 [3] 摘要 |
| [15] | Cotelli M, Manenti R, Brambilla M, et al. Anodal tDCS during face-name associations memory training in Alzheimer's patients[J]. Front Aging neurosci, 2014, 6:38. 本文引用 [3] 摘要 |
| [16] | 康蓉蓉. 重复经颅直流电刺激治疗阿尔茨海默病及轻度认知障碍疗效的Meta分析[D]; 大连医科大学, 2020. |
| [17] | Majdi A, Van Boekholdt L, Sadigh-Eteghad S, et al. A systematic review and meta-analysis of transcranial direct-current stimulation effects on cognitive function in patients with Alzheimer's disease[J]. Molecul Psychiat, 2022, 27(4):2000-2009. |
| [18] | Teselink J, Bawa KK, Koo GK, et al. Efficacy of non-invasive brain stimulation on global cognition and neuropsychiatric symptoms in Alzheimer's disease and mild cognitive impairment: A meta-analysis and systematic review[J]. Ageing Res Rev, 2021, 72:101499. |
| [19] | Moher D, Liberati A, Tetzlaff J, et al. 系统综述和荟萃分析优先报告的条目:PRISMA声明[J]. 中西医结合学报, 2009, 7(9):889-896. |
| [20] | 中国痴呆与认知障碍诊治指南写作组, 中国医师协会神经内科医师分会认知障碍疾病专业学组. 2018中国痴呆与认知障碍诊治指南(五):轻度认知障碍的诊断与治疗[J]. 中华医学杂志, 2018, 98(17): 1294-1301. |
| [21] | Mckhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease[J]. Neurol, 1984, 34(7): 939-944. |
| [22] | Gangemi A, Colombo B, Fabio RA, et al. Effects of short- and long-term neurostimulation (tDCS) on Alzheimer's disease patients: two randomized studies[J]. Aging Clin Experiment Res, 2021, 33(2):383-390. |
| [23] | Khedr EM, Salama RH, Abdel Hameed M, et al. Therapeutic Role of Transcranial Direct Current Stimulation in Alzheimer Disease Patients: Double-Blind, Placebo-Controlled Clinical Trial[J]. Neurorehabil Neural Repair, 2019, 33(5):384-394. 本文引用 [2] 摘要 |
| [24] | Im JJ, Jeong H, Bikson M, et al. Effects of 6-month at-home transcranial direct current stimulation on cognition and cerebral glucose metabolism in Alzheimer's disease[J]. Brain stimulat, 2019, 12(5):1222-1228. |
| [25] | 王东, 贾颐, 卢春晖, 等. 经颅直流电刺激治疗阿尔茨海默病临床疗效观察[J]. 神经损伤与功能重建, 2016, 11(6):509-511. |
| [26] | Khedr EM, Gamal NF, El-Fetoh NA, et al. A double-blind randomized clinical trial on the efficacy of cortical direct current stimulation for the treatment of Alzheimer's disease[J]. Front Aging neurosci, 2014, 6:275. 本文引用 [2] 摘要 |
| [27] | Gonzalez PC, Fong KNK, Brown T, et al. Transcranial direct current stimulation as an adjunct to cognitive training for older adults with mild cognitive impairment: A randomized controlled trial[J]. Ann Phys rehabil Med, 2021, 64(5):101536. |
| [28] | Fileccia E, Di Stasi V, Poda R, et al. Effects on cognition of 20-day anodal transcranial direct current stimulation over the left dorsolateral prefrontal cortex in patients affected by mild cognitive impairment: a case-control study[J]. Neurol sci, 2019, 40(9):1865-1872. 本文引用 [2] 摘要 |
| [29] | 胡荣亮, 陈颂玲, 任雪芹, 等. 经颅直流电刺激对遗忘型轻度认知功能障碍患者应用效果[J]. 深圳中西医结合杂志, 2020, 30(10):4-5. |
| [30] | 胡荣亮, 陈卓铭, 冯尚武, 等. 经颅直流电刺激小脑对遗忘型轻度认知功能障碍患者言语工作记忆能力的影响[J]. 中华物理医学与康复杂志, 2016, 38(4): 267-271. |
| [31] | Lu H, Chan SSM, Chan WC, et al. Randomized controlled trial of TDCS on cognition in 201 seniors with mild neurocognitive disorder[J]. Ann Clin Transl Neurol, 2019, 6(10): 1938-1948. |
| [32] | Stonsaovapak C, Hemrungro JS, Terachinda P, et al. Effect of Anodal Transcranial Direct Current Stimulation at the Right Dorsolateral Prefrontal Cortex on the Cognitive Function in Patients With Mild Cognitive Impairment: A Randomized Double-Blind Controlled Trial[J]. Arch Phys Med Rehabil, 2020, 101(8):1279-1287. |
| [33] | Hoy KE, Emonson MR, Arnold SL, et al. Testing the limits: Investigating the effect of tDCS dose on working memory enhancement in healthy controls[J]. Neuropsychol, 2013, 51(9):1777-1784. |
| [34] | Chan MMY, Yau SSY, Han YMY, et al. The neurobiology of prefrontal transcranial direct current stimulation (tDCS) in promoting brain plasticity: A systematic review and meta-analyses of human and rodent studies[J]. Neurosci Biobehav Rev, 2021, 125:392-416. 本文引用 [1] 摘要 |
| [35] | Dedoncker J, Brunoni AR, Baeken C, et al. A Systematic Review and Meta-Analysis of the Effects of Transcranial Direct Current Stimulation (tDCS) Over the Dorsolateral Prefrontal Cortex in Healthy and Neuropsychiatric Samples: Influence of Stimulation Parameters[J]. Brain stimulat, 2016, 9(4):501-517. |
| [36] | Brunoni AR, Moffa AH, Fregi F, et al. Transcranial direct current stimulation for acute major depressive episodes: meta-analysis of individual patient data[J]. Br J psy, 2016, 208(6):522-531. |
| [37] | Chen W, Liang JF, Jiang LF, et al. Clinical study on the treatment of Alzheimer's disease by traditional Chinese and western medicine[J]. Chin J Chin Med, 2015, 30(2): 265-268. |
| [38] | Varghese T, Sheelakumari R, James JS, et al. A review of neuroimaging biomarkers of Alzheimer's disease[J]. Neurol Asia, 2013, 18(3):239-248. 本文引用 [1] 摘要 |
| [39] | Li M, Long C, Yang L, et al. Hippocampal-prefrontal circuit and disrupted functional connectivity in psychiatric and neurodegenerative disorders[J]. BioMed Res Internat, 2015, 2015:810548. |
| [40] | Rodella C, Bernini S, Panzarasa S, et al. A double-blind randomized controlled trial combining cognitive training (CoRe) and neurostimulation (tDCS) in the early stages of cognitive impairment[J]. Aging Clin Exp Res, 2022, 34(1):73-83. |
| [41] | Das N, Spence JS, Aslan S, et al. Cognitive Training and Transcranial Direct Current Stimulation in Mild Cognitive Impairment: A Randomized Pilot Trial[J]. Front Neurosci, 2019, 13:307. |
| [42] | Yun K, Song IU, Chung YA, et al. Changes in cerebral glucose metabolism after 3 weeks of noninvasive electrical stimulation of mild cognitive impairment patients[J]. Alzheimers Res Ther, 2016, 8(1):49. |